Laparoscopic cervical Mersilene tape insertion is a surgical procedure used to treat cervical incompetency, a condition where the cervix is unable to stay closed during pregnancy, leading to a risk of preterm birth or miscarriage. The procedure involves placing a Mersilene tape, a type of non-absorbable suture material, around the cervix to provide additional support and help maintain the pregnancy until term.
Procedure Overview
- Anesthesia: The procedure is typically performed under general anesthesia, ensuring the patient is comfortable and pain-free during the surgery.
- Laparoscopic Access: Small incisions are made in the abdomen, usually in the umbilical region and lower abdomen. Through these incisions, a laparoscope (a thin tube with a camera) and surgical instruments are inserted.
- Identification of the Cervix: The surgeon identifies the cervix and its surrounding structures using the laparoscope. The bladder may be gently moved out of the way to access the cervix.
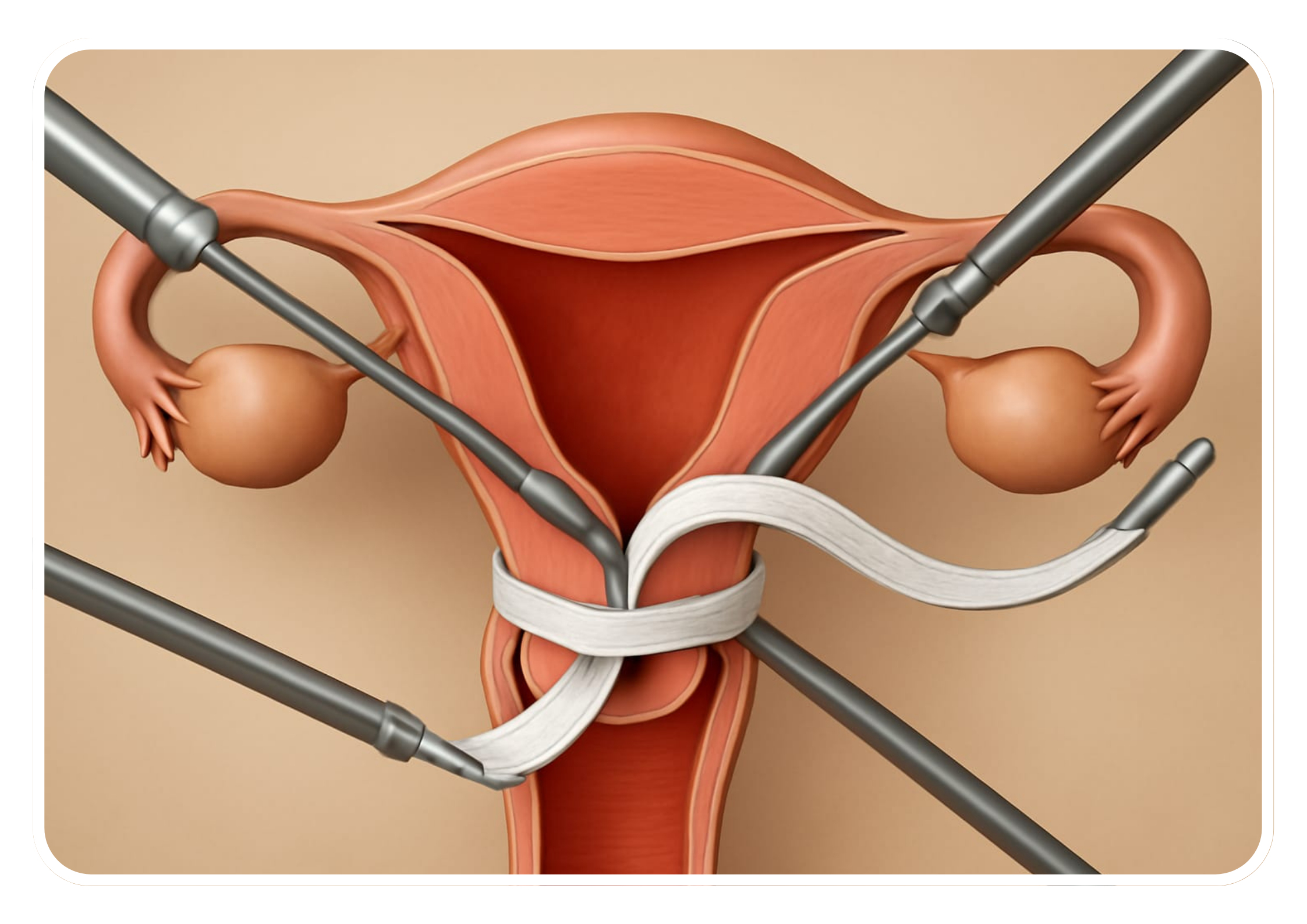
- Tape Insertion: Mersilene tape is passed around the cervix, either anteriorly (in front) or posteriorly (behind), depending on the surgeon’s preference and the patient’s anatomy. The tape is then secured tightly to provide support to the cervix.
- Closure: After the tape is securely placed, the instruments are removed, and the small incisions are closed with sutures or surgical glue.
- Postoperative Care: Patient
Indications
Laparoscopic cervical Mersilene tape insertion is indicated for women with:
- Stress urinary incontinence (SUI) that has not responded to conservative treatments such as pelvic floor exercises, behavioral therapy, or medications.
- SUI characterized by the involuntary leakage of urine during activities that increase intra-abdominal pressure, leading to bladder weakness or dysfunction.
Preoperative Evaluation
Before undergoing laparoscopic cervical Mersilene tape insertion, patients typically undergo a comprehensive preoperative evaluation, including:
- Medical History Review: To understand past health issues and urinary symptoms.
- Physical Examination: To assess overall health and suitability for surgery.
- Urinalysis and Urodynamic Testing: To evaluate bladder function and the extent of incontinence.
- Counseling: Discussing the procedure, risks, benefits, and alternatives, including the possibility of alternative treatments.
Procedure
- Anesthesia: Laparoscopic cervical Mersilene tape insertion is usually performed under general anesthesia in an operating room equipped for laparoscopic surgery.
- Incisions: Several small (typically 0.5 to 1 cm) incisions are made in the lower abdomen, usually below the belly button.
- Trocar Placement: Trocars (hollow tubes) are inserted through the incisions to provide access for the laparoscope and specialized instruments.
- Visualization: A laparoscope is inserted through one of the trocars to provide a magnified view of the pelvic organs, including the bladder and urethra. Carbon dioxide gas is used to inflate the abdominal cavity, creating space for visualization and instrument manipulation.
- Tape Insertion: The Mersilene tape is passed under the urethra and positioned to provide support and compression to the urethral sphincter mechanism. The tape is secured in place using specialized instruments and techniques.
- Adjustment: The tension of the tape may be adjusted to achieve the desired degree of support and continence. The surgeon may perform intraoperative testing, such as cough stress testing, to assess the effectiveness of the tape placement.
- Closure: Once the tape is securely in place and the tension is adjusted, the instruments are removed, and the small incisions are closed with sutures or surgical glue. Dressings may be applied.
Advantages
- Minimally Invasive: Involves smaller incisions, resulting in less postoperative pain, reduced blood loss, shorter hospital stays, and faster recovery times compared to traditional open surgery.
- High Success Rates: Effective in improving or eliminating symptoms of stress urinary incontinence in the majority of patients, with high success rates reported in clinical studies.
- Durable Support: Provides durable support to the urethra, helping to prevent urine leakage during activities that increase intra-abdominal pressure.
Considerations
- Postoperative Care: Patients may experience mild discomfort, urinary frequency, or urinary retention, which typically resolves within a few days to weeks. Patients should avoid strenuous activities and heavy lifting during the recovery period.
- Follow-up: Regular follow-up appointments are necessary to assess postoperative outcomes, monitor for complications, and make any necessary adjustments to the tape tension.
- Risks and Complications: Similar to those of other surgical procedures, including bleeding, infection, urinary retention, urinary tract injury, tape erosion or migration, and recurrence of urinary incontinence. Patients should be informed about these risks during preoperative counseling.
Conclusion
Laparoscopic cervical Mersilene tape insertion is an effective and minimally invasive surgical option for the treatment of stress urinary incontinence in women. When performed by experienced surgeons in appropriately selected patients, Mersilene tape insertion can provide significant improvements in urinary symptoms and quality of life.